
National Eating Disorder Awareness Month: Get The Facts
- Feb 19, 2016
- 8 min read

Eating disorders are so often misunderstood, and I honestly feel that's because the public does not understand them and we never talk about them! Well, since February is National Eating Disorder Awareness Month, it's time to bring ED out of the closet and talk about it, face to face.
Warning: the following post has descriptions of eating disorders, their symptoms and health consequences, and definitions of the actions taken by those who are afflicted. Reader discretion is advised.
What Is An Eating Disorder (ED)?
An eating disorder is "a conditio
n that inhibits an individual's ability to consume food in a manner consistent with good physical and emotional health." These people have an unhealthy relationship with food. EDs can arise from physical, psychological, or mental origins. It's not well understood what exactly caused an eating disorder, but it is known that it is not a choice of the person afflicated (1). EDs are complex and potentially life-threatening mental illnesses (2) that frequently co-exist with other mental illnesses such as anxiety disorders, depression, substance abuse, or other mental illness (3).

What Are The Types of Eating Disorders?
Psychologists use The Diagnosist and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V) to classify mental disorders using a set of criteria. The DSM-V recognizes the following eating disorders (1):
Anorexia Nervosa (AN) - 2 subtypes:
Restrictive Type
Binge/Purging Type
Bulimia Nervosa (BN)
Binge Eating Disorder (BED)
Other Specified Feeding or Eating Disorder (OSFED) - previously known as Eating Disorder Not Otherwise Specified (EDNOS)
Avoidant/Restrictive Food Intake Disorder (ARFID)
Rumination Disorder
Pica
Unspecified Feeding or Eating Disorder
Anorexia Nervosa (AN)
"Anorexia nervosa" was first used in 1873 by Sir William Gill, a physician who had observed this condition in his patients. It comes from Greek, meaning "a nervous loss of appetite." AN is characterized by:
Behavior or activity that limits the number of calories consumed and promotes expenditure of calories in such a way that results in an inability to maintain an acceptable weight needed for good health. These activities include: food restriction, intense/prolonged exercise, laxative/diuretic/enema use, vomiting (1). Individuals will deny that they are hungry, develop 'food rituals' to decrease amount of food consumed (excessive chewing, rearrange food on plate, cut up food into tiny pieces, etc.), and may even consistently avoid mealtimes or situations that involve food (4).
An overwhelming and obsessive anxiety related to one's weight and an intense fear of weight gain. These individuals are obsessed with their weight and are very persistent in their behavior to prevent weight gain. Many individuals with AN are below normal body weight because they are not able to ingest enough calories (1,2).
Distorted perception of body size and an over-emphasis on thinness. These individuals often feel they are never 'thin enough.' Imagine looking into a funhouse mirror at the fair and how different your body looks. This is how a person with anorexia sees themselves on a daily basis. They do not see themselves how they really are (1).
The individual does not consider the consequences of the behavior People suffering from AN are not able to appreciate the severity of their situation. They may be warned repeatedly about how dangerous their low caloric intake is, but they are so focused on their goal of thinness that nothing else is as important (1, 2)
Symptoms/Health Consequences (3,4):
extremely low body weight
food restriction
food rituals
lack of menstruation in girls and women
loss of body hair - leads to growth of downy layer of hair called "lanugo"
muscle loss and weakness
severe dehydration
heart failure due to slow heart rate
fainting and fatigue
reduced bone mass leading to early osteoporosis
According to the National Eating Disorder Awareness Association (NEDA), 5-20% of those who suffer with anorexia nervosa will die. This makes AN the most deadly mental illness (4).
Bulimia Nervosa (BN)
"Bulimia Nervosa" was first defined in 1979 by British psychiatrist Gerald Russell. It comes from Greek meaning "nervous, ravenous hunger." BN is characterized by:
Cycles of restriction followed by bingeing. A binge is consuming a large amount of food at one time. This amount of food is more than a healthy person would consider reasonable. During this binge, the person feels they have lost control over the food they are eating (1).
Recurring episodes of behavior designed to rid the body of calories consumed during the binge (AKA purging). Purging may consist of excessive exercise, vomiting, laxative/enema/or diuretic use. Purging is very dangerous for one's health and it is not effective in shedding the excessive amount of calories consumed in the binge (1).
Negative self-image related to body size and shape. A person suffering from bulimia has self-esteem that is overly related to their body image (5). Like people with anorexia, those with bulimia place their body image as highly important. However, unlike with anorexia, people with bulimia often have a weight that falls within the normal range (1).
Episodes of restricting, bingeing, and purging occur at least once per week over a three month period. As the routine becomes more frequent, it is more difficult for a person to break that cycle. Many individuals suffering from BN have a deep sense of shame related to their behaviors (1).
Symptoms/Health Consequences (5):
evidence of purging: frequent trips to the bathroom after meals, presence of laxative wrappers, signs or smells of vomiting, continued exercise despite injury
evidence of bingeing: large amounts of food disappear in short periods of time
calluses on back of hands and knuckles from self-induced vomiting
swelling of cheeks or jaw
tooth decay and staining (from stomach acids due to vomiting)
chronic irregular bowel movements (from laxative use)
inflammation and possible rupture of esophagus
heart failure (due to electrolyte imbalance)
Binge Eating Disorder (BED):
BED was first descriped in 1995 by Albert Stunkard, a psychiatrist who originally called it "night eating syndrome." It was later changed to Binge Eating Disorder because the episodes do not necessarily occur at night (1). BED is characterized by:
Repeated episodes of bingeing. Similar to BN in this sense. Additionally the episode involes 3 or more of the following characteristics: - eating much more rapidly than normal - eating past the point of being satiated, to uncomfortably full - eating large amounts when not physically hungry - eating alone because of embarrassement at amount being eaten - feeling disgusted with oneself, depressed, or very guilty after binge (6)
Binges are not followed by purging or any method to compensate for calories consumed. This is what distinguishes BED from BN (1).
Bingeing episodes occur at least once per week for at least a 3 month period.
Severe anxiety and anguish/guilt related to binge-eating.
Symptoms/Health Consequences:
high blood pressure
Type 2 Diabetes
heart disease
high cholesterol
sleep apnea
joint pain
possible weight gain
possible obesity (6)
Other Specified Feeding or Eating Disorder (OSFED)/EDNOS
This ED was first described in 1980 in DSM-III. This is characterized by irregular eating patterns but does not meet the full criteria for the other eating disorders listed above. Examples:
Atypical Anorexia Nervosa: the individual meets the other criteria for AN, but is within or above normal weight.
Bulimia Nervosa (of low frequency and/or limited duration): meets the criteria for BN, but the binge-purge cycles are less often than once per week.
Binge-eating disorder (of low frequency and/or limited duration): same concept as #2
Purging disorder: purging activities desided to keep body weight or shape but without bingeing
Night eating syndrome: consuming unusually large amounts of food after evening meal or when waking up during the night (1).
Avoidant/Restrictive Food Intake Disorder (ARFID)
Prior to DSM-V, this was known as Feeding Disorder of Infancy or Early Childhood. However, it can continue into adulthood. It is characterized by:
Failure to consume enough food to maintain caloric requirements for energy or growth: this includes a lack of interest in eating, negative sensory qualities associated with food (texture, smell), fear of choking, gagging or becoming ill after eating food.
The eating behavior cannot be attributed to inadequate food supply, other medical condition, or cultural observances.
The disorered eating pattern occurs independently of diagnosis of another ED and body image distortion is not present (1).
Rumination Disorder
"Rumination" comes from the Latin "to chew the cud." This was first clinically described in 1618 by an anatomist. This condition is defined as regurgitating of food (voluntary or involuntary return of partially digested food from the stomach to the mouth). The food may be regurgitated, chewed again, swallowed, or spit out. This behavior occurs independently of AN, BN, BED, or ARFID (1).
Pica
Pica comes from the Latin word for magpie, a bird that is said to eat neraly everything. It was first identified in 1563. In the 1800's, it was used by black slaves, by eating clay in order to compensate for their poor diet. This behavior continues today as parts of some spiritual and medicinal rituals in some cultures. Individuals with Pica consume non-food materials that have no nutritional benefit such as: chalk, wood, soil, coal, charcoal, ash, clay, ice, paper, starch, soap, textiles, gum, hair, metal, or gravel. Pregnant women have been known to crave non-food items, but this does not necessarily neccesitate a diagnosis of pica (1).
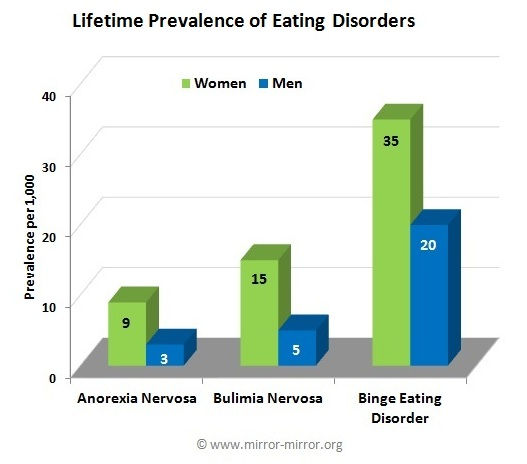
How Common Are Eating Disorders?
In the United States, it is estimated that 20 million women and 10 million men suffer from an eating disorder at some time in their lives. For various reason, many cases are not reported. There are many individuals who struggle with poor body-image and disordered eating patterns and behaviors, that do not have a clinical eating disorder.
The rate of development of eating disorders has been increasing since 1950, with the incidence of bulimia in 10-39 year old women tripling between 1988-1993. This may be due, in part, to an increased understanding of diagnosis and people seeking help.
Despite the high prevalence of eating disorders, there continues to be a lack of funding for research. According to the NIH, money spent on researching Alzheimer's averaged $88 per affected peron in 2011, $81 for schizophrenia, and $44 for autism. For eating disorders, the average amount of research dollars spent per affected person was only $0.93. The table below shows the total research money spent in 2011 (2).

Chart adapted from NEDA's website (2)
Our Society Promotes A Drive For Thinness
A study in 1991 found that 42% of 1st-3rd grade girls want to be thinner
Over 1/2 of teenage girls and 1/3 of teenage boys use unhealthy weight control methods like skipping meals, smoking, vomiting, using laxatives, and fasting, per a 2005 study
The average BMI of Miss America winners has decreased from 22 in the 1920s to 16.9 in the 2000s
The average American woman is 5'4" and weighs 165 lbs. The average Miss America winner is 5'7" and weighs only 121 lbs.
47% of American elementary school girls who read magazines say the pictures make them want to lose weight
Girls who diet frequently are 12x more likely to binge compared to girls who don't diet
95% of all dieters will regain their lost weight in 1-5 years
81% of 10 year olds are afraid of being fat (2)
80% of 13 year old girls have dieted
50% of girls between the ages of 13 and 15 believe they are overweight (7)
Mortality rates are 4% for anorexia, 3.9% for bulimia, and 5.2% for OSFED/EDNOS (8)
Given the above, eating disorders are much more common than most people think or realize. Yet, research dollars to help individuals affected are miniscule compared to other mental illnesses. It's time to bring eating disorders forward. Let's help others!
For more information on eating disorders check out: NEDA and Mirror-Mirror
Resources:
1) http://www.mirror-mirror.org/def.htm
2) http://www.nationaleatingdisorders.org/get-facts-eating-disorders
3) http://www.nimh.nih.gov/health/publications/eating-disorders-new-trifold/index.shtml
4) http://www.nationaleatingdisorders.org/anorexia-nervosa 5) http://www.nationaleatingdisorders.org/bulimia-nervosa
6) http://www.nationaleatingdisorders.org/binge-eating-disorder
7) http://www.mirror-mirror.org/anorexia-statistics.htm
8) http://www.nationaleatingdisorders.org/mortality-and-eating-disorders



























Comments